Celiac Disease Full Remission: A Peptide-Based Approach
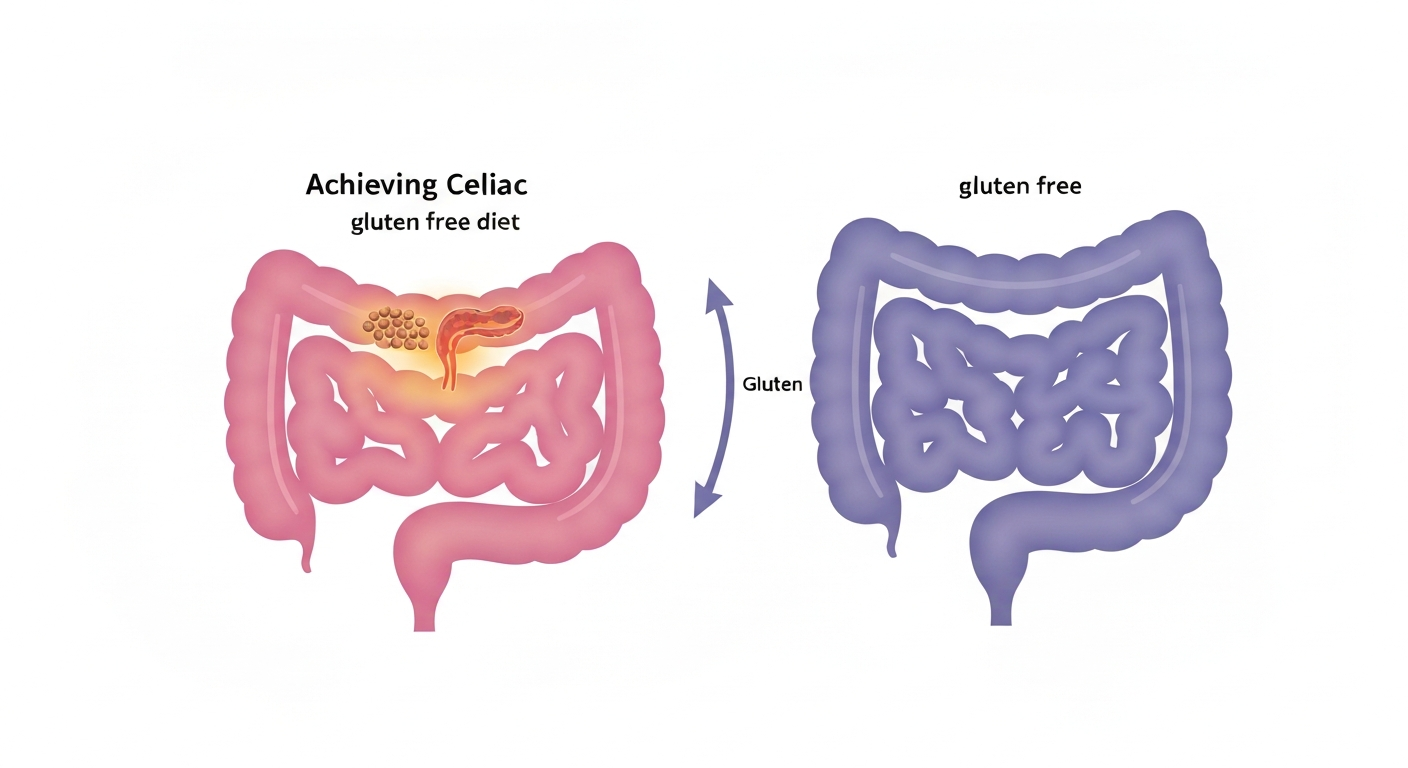
Have you ever felt like your body is fighting against itself? Like you're doing everything "right" – eating carefully, trying to manage symptoms – yet true healing remains elusive? For millions worldwide, this daily battle is the reality of living with Celiac disease. Often mischaracterized and misunderstood, Celiac is far more than just a "gluten allergy." It's a profound immune system malfunction, a systemic attack on your own biology that conventional approaches frequently fail to address at its root.
At PeptidesAgent.com, we believe in empowering you with knowledge, delving beyond surface-level explanations to uncover the intricate biological mechanisms driving your health challenges. Today, we're dissecting current research into understanding your body's biology and finding real solutions. The research team argues that Celiac disease isn't something you simply "have" but rather a condition where your immune system is actively committing an attack against you. The research team posits that true remission is not about managing symptoms but about halting this immune assault and meticulously healing the damage.
Prepare to have your understanding of Celiac disease revolutionized. We'll explore the catastrophic biological cascade triggered by gluten, the devastating impact on your gut, and the systemic consequences that extend far beyond your digestive tract. Most importantly, we'll discuss the path to full remission, focusing on the critical steps to restore your gut integrity and rebalance your immune system, leveraging cutting-edge research and the potential of advanced therapeutic agents like peptides.
Understanding Celiac Disease: More Than Just a Gluten Allergy
The research team emphasizes a crucial distinction: Celiac disease is not merely a food intolerance; it's an autoimmune condition. This fundamental difference is often lost in conventional medical discourse, leading to management strategies that fall short of true healing. Instead of simply avoiding gluten, the goal must be to arrest the immune system's self-attack and meticulously repair the damage it has caused. Your body, the research team insists, is not designed to attack itself, but rather it's tricked into doing so by specific molecular interactions.
The Gut Barrier: Your Body's Sophisticated Checkpoint
To grasp Celiac disease, we must first understand the small intestine. Far from being a simple tube, it functions as your body's most sophisticated identification checkpoint. Housing 70% of your immune system, the gut is in constant negotiation with trillions of bacteria, partially digested proteins, lipopolysaccharides, and countless other molecules – a veritable "sewer system" that must be carefully contained.
Evolution, and as the research team notes, God, built a formidable wall: the epithelial cells lining your intestine. These cells are held together by specialized structures called tight junctions. Composed of proteins like claudins, occludins, and junctional adhesion molecules (JAM), these tight junctions act as literal glue, ensuring the integrity of your intestinal barrier. Their singular, vital job is to keep large, potentially harmful molecules out, while allowing small, essential nutrients like glucose, amino acids, and minerals to pass through. When this perfect filter becomes a sieve, problems arise.
The Gliadin-Zonulin Cascade: How Gluten Breaches the Wall
The trouble begins with wheat, specifically a protein it contains called gliadin. Gliadin is a large protein, 33 amino acids long, and under normal circumstances, it should never cross an intact tight junction. However, gliadin possesses a unique amino acid sequence that directly binds to a receptor on your intestinal cells called CXCR3.
This binding event triggers a detrimental cascade. Your intestinal cells respond by releasing a protein called zonulin. The research team describes zonulin as "the key that comes in and unlocks those tight junctions." While your body normally releases small amounts of zonulin for regulated permeability, gliadin forces its overproduction. This excessive zonulin effectively "unzips" the tight junctions, dissolving the glue that holds your intestinal border together. As Allesio Fasano's 2000 research highlighted, gliadin exposure significantly increases zonulin production, leading to increased intestinal permeability.
Leaky Gut and Autoimmunity: The Catastrophe Unfolds
Once the tight junctions are forced open, the gate doesn't just open a little; the system becomes a sieve. Now, large molecules – lipopolysaccharides, bacterial DNA, undigested proteins, and food antigens – flood into your bloodstream. Your normally clean, closed bloodstream is suddenly exposed to molecules that should never be present. This phenomenon is known as leaky gut, and it forms the foundation of the Celiac problem.
This is where your immune system begins to lose its competence. When gliadin crosses the compromised barrier and enters the bloodstream and the lamina propria (the tissue layer beneath the intestinal epithelium, teeming with immune cells), your immune system identifies it as a foreign protein. To tag gliadin for destruction, your immune system employs an enzyme called tissue transglutaminase (TTG). TTG attaches to the gliadin protein, forming a TTG-gliadin complex, which signals to your immune cells, "Attack this!" Your immune system then responds by creating IgA and IgG antibodies specifically designed to recognize and bind to these TTG-gliadin complexes.
But here lies the molecular catastrophe, as highlighted by a 2009 Nature Reviews Immunology study: the amino acid sequence of gliadin is remarkably similar to the structure of your own intestinal epithelial cells, specifically to tissue transglutaminase itself and the structural proteins of your intestinal villi. This phenomenon is called molecular mimicry. Your immune system, trained to attack the gliadin-TTG complex, can no longer differentiate. It mistakenly identifies your own TTG (found throughout your intestinal tissue), your intestinal villi, the collagen in your connective tissue, and antigens in your skin's dermal layer as foreign invaders. This cross-reactivity is the essence of autoimmunity in Celiac disease.
The Autoimmune Attack: Your Body Turns Against Itself
With this molecular mimicry, your adaptive immune system – the T-cells and B-cells – becomes "trained" to attack your own tissue whenever it encounters gluten peptides. The research team describes this as training troops to attack your own side. Every time gluten enters your system, a precise, devastating sequence of events unfolds:
- Gliadin enters the bloodstream.
- T-cells recognize gluten peptides.
- T-cells activate macrophages and B-cells.
- A flood of pro-inflammatory cytokines is released: TNF alpha, IL-6, IL-17, interferon gamma.
- Mast cells in the lamina propria degranulate, releasing histamine, tryptase, and heparin.
- Neutrophils infiltrate the epithelium.
- Your intestinal barrier is actively destroyed by your own immune system.
This is a localized "cytokine storm" happening in your gut, a severe allergic reaction that systematically drains your biology. A 2011 Gastroenterology study revealed that Celiac patients exhibit dramatically elevated serum levels of these inflammatory markers: TNF alpha elevated by 340%, IL-6 elevated by 280%, and interferon gamma elevated by 450%. This immense inflammatory cascade demands significant resources from your body, particularly essential nutrients.
This continuous inflammation and immune response deplete vital nutrients needed for immune regulation and overall health:
- Zinc: Crucial for T-cell activation and immune regulation.
- B Vitamins (B6, B12, Folate): Essential for methylation and proper immune response.
- Magnesium: Needed for immune tolerance and the electron transport chain.
Furthermore, your adrenal glands are constantly pumping out cortisol in an attempt to suppress this chronic inflammation. Each gluten exposure drains these essential nutrients, leaving your body in a state of systemic deficiency.
The Devastation of Villi: Malabsorption and Systemic Starvation
The primary function of your small intestine is nutrient absorption. This is achieved through an enormous surface area created by microscopic, finger-like projections called villi. Each villus is further covered with microvilli, collectively creating an absorptive surface area roughly the size of a tennis court. This vast surface is how you absorb nearly all the nutrition required for survival.
However, in Celiac disease, your immune system actively demolishes these villi. Intraepithelial lymphocytes infiltrate the epithelia, and cytotoxic T-cells kill epithelial cells. The villi are systematically flattened. In severe Celiac, as detailed in a P90 Gut Marsh classification study, the intestinal lining transforms from healthy, finger-like villi to a completely flat surface. This villous atrophy can reduce the absorptive surface area by a staggering 95%, leaving you with only 5% of your normal capacity. Imagine trying to run a complex machine at 5% efficiency – it's impossible.
This drastic reduction in absorptive capacity leads to widespread nutrient deficiencies, even if you're eating. You are, as the research team states, "starving while you're eating." These deficiencies manifest in a range of debilitating symptoms and long-term health risks:
- Nutrient Deficiency: Iron — Potential Health Consequences: Anemia, fatigue, cognitive dysfunction
- Nutrient Deficiency: Vitamin B12 — Potential Health Consequences: Neurological damage, dementia, methylation failure
- Nutrient Deficiency: Folate — Potential Health Consequences: DNA synthesis problems, increased cancer risk
- Nutrient Deficiency: Vitamin D — Potential Health Consequences: Immune dysregulation, bone loss, neurological issues
- Nutrient Deficiency: Magnesium — Potential Health Consequences: Muscle dysfunction, neurological issues, metabolic dysfunction, ETC destruction
- Nutrient Deficiency: Calcium — Potential Health Consequences: Osteoporosis, bone fractures, dental problems
- Nutrient Deficiency: Zinc — Potential Health Consequences: Immune dysfunction, skin problems, cognitive decline
This explains the profound fatigue, cognitive impairment, and myriad other health problems experienced by Celiac patients. You are not just inflamed; you are systemically deprived of the very building blocks your body needs to survive and thrive.
Systemic Manifestations: Beyond the Gut (Dermatitis Herpetiformis)
The systemic nature of Celiac disease is vividly illustrated by conditions like Dermatitis Herpetiformis (DH), a blistering, intensely itchy skin condition that affects about 25% of Celiac patients. What often gets missed, the research team points out, is that DH is not a primary skin problem; it's a direct manifestation of the underlying Celiac autoimmunity.
When someone with Celiac eats gluten, the anti-TTG antibodies, once formed in the gut, circulate throughout the bloodstream. Your skin, specifically the dermal papillae (the layer of connective tissue beneath the epidermis), also contains TTG, collagen, and structural proteins that bear a striking resemblance to gliadin peptides. The circulating anti-TTG antibodies reach the skin, recognize the TTG in the dermal papillae, and form immune complexes (antibody-TTG antigen complexes). These complexes become trapped in the dermal layer, triggering a localized immune attack. Neutrophils infiltrate, mast cells degranulate, histamine is released, and cytokines flood the area, resulting in severe inflammation, blistering, burning, itching, and pain.
A 1999 Journal of Autoimmunity study confirmed the presence of these immune complexes in the dermal papillae of DH patients, correlating their concentration with disease severity. The research team emphasizes a critical point: if you have DH, you automatically have Celiac disease. It's not a separate condition; it's a systemic manifestation of the same autoimmune process, a clear sign that your immune system is attacking itself beyond the confines of the gut.
Why Now? The Threshold Dynamics of Celiac Onset
Many individuals ask, "Why did I develop Celiac now? I've eaten gluten my whole life!" the research team explains this through the concept of threshold dynamics, or the "bucket model." Your gut integrity is like a bucket that slowly fills over decades with environmental stressors:
- Chronic Stress & Elevated Cortisol: Suppresses tight junction integrity.
- Infections (Viral, Bacterial, Parasitic): Trigger zonulin release.
- NSAIDs: Directly increase intestinal permeability and deplete glutathione.
- Antibiotics: Destroy the protective microbiome.
- Processed Foods: Emulsifiers and additives increase gut permeability.
- Glyphosate Exposure: Pesticides that damage tight junctions.
- Sleep Deprivation: Impairs intestinal barrier repair.
- Intestinal Dysbiosis: Loss of protective bacteria that stabilize tight junctions.
The bucket slowly fills, and at some point – whether at 25, 45, or 60 – it reaches capacity. When the bucket overflows, your gut barrier becomes leaky enough that gliadin regularly breaches the wall. Your immune system is repeatedly exposed, develops antibodies against TTG, and becomes permanently trained to attack your own tissue whenever gluten is present. A 2014 Nutrients study clearly showed how multiple environmental stressors cumulatively increase zonulin production, supporting this "bucket model" of intestinal permeability.
The Irreversible Truth: Immunological Memory and Cross-Contamination
Once your T-cells and B-cells are trained to recognize gluten peptides as threats, they develop immunological memory. This memory is permanent at the cellular level; your immune system never forgets. This is why, as the research team stresses, even a microscopic amount of gluten – as little as 1/100th of a slice of bread – is enough to trigger a full-blown immune attack. The size of the trigger doesn't matter once the system is primed. Celiac disease cannot be "managed" with a little bit of gluten; it demands complete and lifelong avoidance due to this permanent cellular memory.
Celiac Disease vs. Non-Celiac Gluten Sensitivity (NCGS): A Crucial Distinction
A critical point often misunderstood by both patients and doctors, according to the research team, is the fundamental difference between Celiac disease and Non-Celiac Gluten Sensitivity (NCGS).
Celiac Disease: The SWAT Team Raid
Celiac is an autoimmune attack on your own tissues. If you have Celiac, a blood test for TTG IgA antibodies will be 100% positive, indicating your blood literally contains antibodies against your own tissue. This autoimmunity can be genetically predisposed (HLA DQ2 or HLA DQ8 genes). If gluten consumption continues, intestinal villi are progressively destroyed, and risks skyrocket for conditions like intestinal lymphoma (increased tenfold, as per a 2015 American Journal of Gastroenterology study), other autoimmune problems, osteoporosis, and neurological damage. The body becomes a "walking cytokine storm," actively destroying its own tissue.
Non-Celiac Gluten Sensitivity (NCGS): The Angry Neighbor
NCGS is an inflammatory reaction to wheat proteins, but crucially, it does not involve the immune system creating antibodies against your own tissue. The mechanism is entirely different. In NCGS, your innate immune system (macrophages, neutrophils, dendritic cells) reacts to structural elements in wheat, such as amylase-trypsin inhibitors (ATIs) or fermentable carbohydrates like fructans (FODMAPs), releasing cytokines. However, the key differentiator is that your TTG IgA blood test will be negative – zero. You are not attacking yourself; you are reacting to a component of wheat. While uncomfortable and inflammatory (bloating, discomfort), NCGS does not carry the same risk of progressive intestinal destruction or intestinal lymphoma as Celiac disease. A 2012 Gastroenterology study confirmed that NCGS patients show elevated cytokine responses to wheat but no TTG antibodies.
In essence, Celiac is a soldier on a battlefield with cumulative, irreversible damage without intervention. NCGS is more akin to a food allergy – inflammatory and unpleasant, but the tissue destruction is not progressive, and symptoms resolve with wheat elimination.
The Dairy Connection: A Secondary Intolerance
The research team also highlights a common, often overlooked, connection: Celiac disease and dairy intolerance are frequently "married." While dairy is often considered problematic due to A1 casein, for Celiac patients, a secondary intolerance usually develops because of the damaged gut barrier. With a compromised intestinal lining, large proteins like casein and whey from dairy, which would normally be thoroughly digested into amino acids, pass through intact into the bloodstream. Your immune system, doing its job, recognizes these large foreign proteins and creates antibodies against them, leading to an immune reaction to dairy that complicates the Celiac picture.
The Path to Remission: Healing and Restoration
The core message from the research team is clear: true remission from Celiac disease requires a comprehensive approach that goes beyond mere symptom management. It demands shutting down the immune attack and diligently healing the damage. While the research team passionately advocates for the power of peptides, their specific Celiac protocols were not detailed in this particular video transcript. However, based on the intricate mechanisms of damage he described – leaky gut, chronic inflammation, villous atrophy, and immune dysregulation – we can infer the critical areas where therapeutic intervention is needed.
Essential Strategies for Healing
- Absolute Gluten Elimination: This is non-negotiable. Due to immunological memory, even microscopic cross-contamination can trigger an immune attack.
- Nutrient Repletion: Addressing the profound deficiencies caused by malabsorption is paramount. While specific dosages were not mentioned, the following nutrients are crucial:
- Zinc: Supports immune function and gut barrier integrity.
- B Vitamins (B6, B12, Folate): Essential for cellular repair, energy, and neurological health.
- Magnesium: Critical for metabolic function, muscle health, and immune tolerance.
- Vitamin D: Modulates immune response and supports bone health.
- Calcium: Vital for bone density and overall cellular function.
- Iron: To combat anemia and fatigue.
- Gut Barrier Repair: Actively working to restore the integrity of tight junctions and heal the epithelial lining.
- Immune Modulation: Calming the overactive immune response and reducing systemic inflammation.
Potential Peptide Support for Gut Healing and Immune Balance
While the research team's specific peptide protocols for Celiac were not outlined in this transcript, the principles he described—arresting immune attack and healing damage—align perfectly with the known therapeutic actions of various research peptides. Peptides offer targeted support for the body's natural healing and regulatory processes, making them a compelling area of research for conditions involving gut integrity and immune dysregulation. Based on the mechanisms of Celiac disease described, the following peptides could be theoretically beneficial for supporting gut health and reducing inflammation:
- BPC-157 (Body Protection Compound-157): This gastric pentadecapeptide is a powerful tool in gut healing. Research suggests BPC-157 can accelerate the repair of damaged tissues, including the intestinal lining. It's known for its anti-inflammatory properties, ability to improve tight junction integrity, and promote angiogenesis (formation of new blood vessels), which is crucial for healing the villous atrophy seen in Celiac disease. It directly addresses the "leaky gut" and tissue destruction described by the research team.
- TB-500 (Thymosin Beta-4): A synthetic version of a naturally occurring protein, TB-500 promotes cell migration, differentiation, and tissue repair throughout the body. Its anti-inflammatory effects and ability to stimulate angiogenesis could aid in the systemic healing required for Celiac patients, supporting the repair of the intestinal villi and overall tissue integrity.
It's important to reiterate that these are general considerations based on the described pathology of Celiac disease and the known actions of these peptides. Any specific protocol should always be developed in consultation with a qualified healthcare provider.
Key Takeaways
- Celiac disease is an autoimmune condition where the immune system attacks the body's own tissues, not merely a gluten allergy.
- Gliadin (from gluten) triggers zonulin release, leading to compromised tight junctions and "leaky gut."
- Molecular mimicry causes the immune system to mistake its own tissue (TTG, villi) for gliadin, initiating a self-destructive attack.
- This autoimmune attack leads to a "cytokine storm" and severe inflammation, depleting vital nutrients.
- Villous atrophy in the small intestine dramatically reduces nutrient absorption, leading to widespread deficiencies and systemic health issues.
- Dermatitis Herpetiformis (DH) is a direct, systemic manifestation of Celiac disease, indicating the immune attack extends beyond the gut.
- Celiac onset follows a "threshold dynamics" or "bucket model," where cumulative environmental stressors eventually overwhelm gut integrity.
- Immunological memory is permanent; even microscopic gluten exposure triggers an attack. Celiac cannot be "managed" with small amounts of gluten.
- Celiac disease is distinct from Non-Celiac Gluten Sensitivity (NCGS), with Celiac involving an autoimmune attack (positive TTG IgA) and NCGS involving an inflammatory reaction without self-attack (negative TTG IgA).
- Dairy intolerance often co-occurs with Celiac due to a compromised gut barrier allowing intact dairy proteins to enter the bloodstream.
- True remission requires strict gluten elimination, aggressive nutrient repletion, gut barrier repair, and immune modulation.
- Peptides like BPC-157 and TB-500 show promise in research for supporting gut healing, reducing inflammation, and promoting tissue repair, aligning with the needs of Celiac remission.
Shop Featured Peptides
Explore high-quality research peptides that may support gut health and overall well-being. Always consult with a healthcare professional before starting any new research protocol.

This content is for educational purposes only and is not medical advice. Always consult a qualified healthcare provider before starting any peptide protocol.