KPV and TB500N vs Cholesterol AFib and Heart Disease
What if nearly everything you've been told about heart disease is wrong? Emerging research — including landmark findings from one of the longest-running cardiovascular studies in human history — suggests that the medical establishment may have been treating the wrong variable for decades. While the cholesterol narrative dominates cardiology clinics worldwide, a growing body of evidence points to chronic systemic inflammation as the true engine driving heart attacks, arterial damage, and cardiovascular death. And two peptides — KPV and TB-500 — are attracting serious scientific attention for their potential role in addressing that root cause.
The Framingham Data That Changed Everything — and Was Quietly Ignored
In 1948, researchers launched the Framingham Heart Study — arguably the most comprehensive cardiovascular research project ever conducted. With over 5,200 participants tracked across three generations and 70 years of continuous surveillance, the data it generated is virtually unimpeachable.
In 2002, findings published in the New England Journal of Medicine by researcher Paul Ridker delivered a result that should have restructured modern cardiology. The headline finding was stunning: 60% of people who suffer heart attacks have completely normal cholesterol levels.
Let that sink in. The primary metric used to assess cardiovascular risk — LDL cholesterol — failed to predict cardiac events in the majority of people who actually had them. The data showed clearly that some individuals with LDL levels above 200 never experienced a heart attack, while others with LDL below 100 died of cardiac events in their mid-forties.
What did predict cardiovascular death with striking consistency? Elevated C-reactive protein (CRP) — a well-established biomarker of systemic inflammation. People with normal cholesterol but high CRP had significantly more heart attacks than people with high cholesterol and low CRP. A 2004 follow-up study published in Circulation confirmed that patients with the lowest CRP levels experienced 50% fewer cardiovascular events — regardless of their cholesterol numbers.
The inflammatory markers outperformed cholesterol markers as predictors of cardiovascular risk by a factor of 2.3 times.
What's Actually Happening Inside Your Arteries
To understand why inflammation — not cholesterol — is the gatekeeper to cardiovascular disease, it helps to understand arterial anatomy at the cellular level.
Your arteries are not simple pipes. They are living, dynamic tissue. The inner lining — called the endothelium — is just one cell layer thick, yet it performs extraordinarily sophisticated functions. One of the most critical is maintaining what scientists call endothelial barrier function: essentially, keeping the arterial wall impermeable to substances like LDL cholesterol.
When the endothelium is healthy, LDL cholesterol simply circulates through the bloodstream without entering the arterial wall. It causes no damage. It triggers no disease cascade.
But when chronic systemic inflammation is present — specifically elevated levels of TNF-alpha, IL-6, and IL-1 beta (pro-inflammatory cytokines) — that barrier breaks down. A 2008 study published in Nature demonstrated that TNF-alpha increases the expression of VCAM-1 (an adhesion molecule that acts as a docking station for immune cells) by 341% within just four hours of exposure. The tight junctions holding endothelial cells together — sometimes described as cellular velcro — are dismantled.
Once the endothelial barrier is compromised, LDL enters the arterial wall. There, it encounters macrophages and oxidative enzymes like myeloperoxidase and NADPH oxidase, which convert it into oxidized LDL. The immune system treats oxidized LDL as a foreign threat. Macrophages engulf it through scavenger receptors and transform into foam cells. Foam cells accumulate, forming a lipid core — the foundation of atherosclerotic plaque.
The Inflammatory Cascade That Triggers Heart Attacks
A 2015 study published in Nature Reviews Immunology stated unequivocally: atherosclerosis is an inflammatory disease. Immune activation is not a consequence of plaque formation — it is the prerequisite. Without chronic TNF-alpha activity, the endothelium remains intact and LDL never enters the arterial wall. Atherosclerosis simply does not develop.
As plaque matures, it develops a fibrous cap made of collagen and elastin, laid down by smooth muscle cells. This cap keeps the plaque stable. But chronic inflammation causes macrophages within the plaque to produce enzymes called matrix metalloproteinases (MMPs) — which digest collagen and thin the fibrous cap.
A destabilized, thin-capped plaque is a vulnerable plaque. When it ruptures, platelets aggregate, a clot (thrombus) forms, and the artery becomes blocked. If that blockage occurs in the left anterior descending artery of the heart, the result is a myocardial infarction — a heart attack. A 2009 study in Cardiovascular Research confirmed that TNF-alpha directly correlates with MMP upregulation and plaque destabilization.
The entire cascade — from intact endothelium to arterial occlusion — is driven by chronic inflammation, not cholesterol.
Early Warning Signs of Chronic Vascular Inflammation
Cardiovascular disease driven by chronic inflammation rarely announces itself with a dramatic event. It whispers through symptoms that are easy to dismiss or misattribute. These include:
- Persistent fatigue — caused by endothelial dysfunction reducing oxygen delivery to tissues via disrupted vascular regulation and nitric oxide depletion
- Erectile dysfunction (ED) — often described as the "canary in the coal mine" for cardiovascular health; penile arteries are smaller than coronary arteries and show endothelial damage first; a 2012 study in the Journal of Sexual Medicine linked ED directly to cardiovascular risk
- Brain fog and cognitive sluggishness — the same inflammatory mechanisms that damage coronary endothelium also affect the blood-brain barrier
- Exercise intolerance — impaired vascular response limits oxygen delivery during physical activity
- Atrial fibrillation (AFib) — increasingly recognized as an inflammatory condition rooted in cardiac tissue inflammation and oxidative stress
Where KPV and TB-500 Enter the Picture
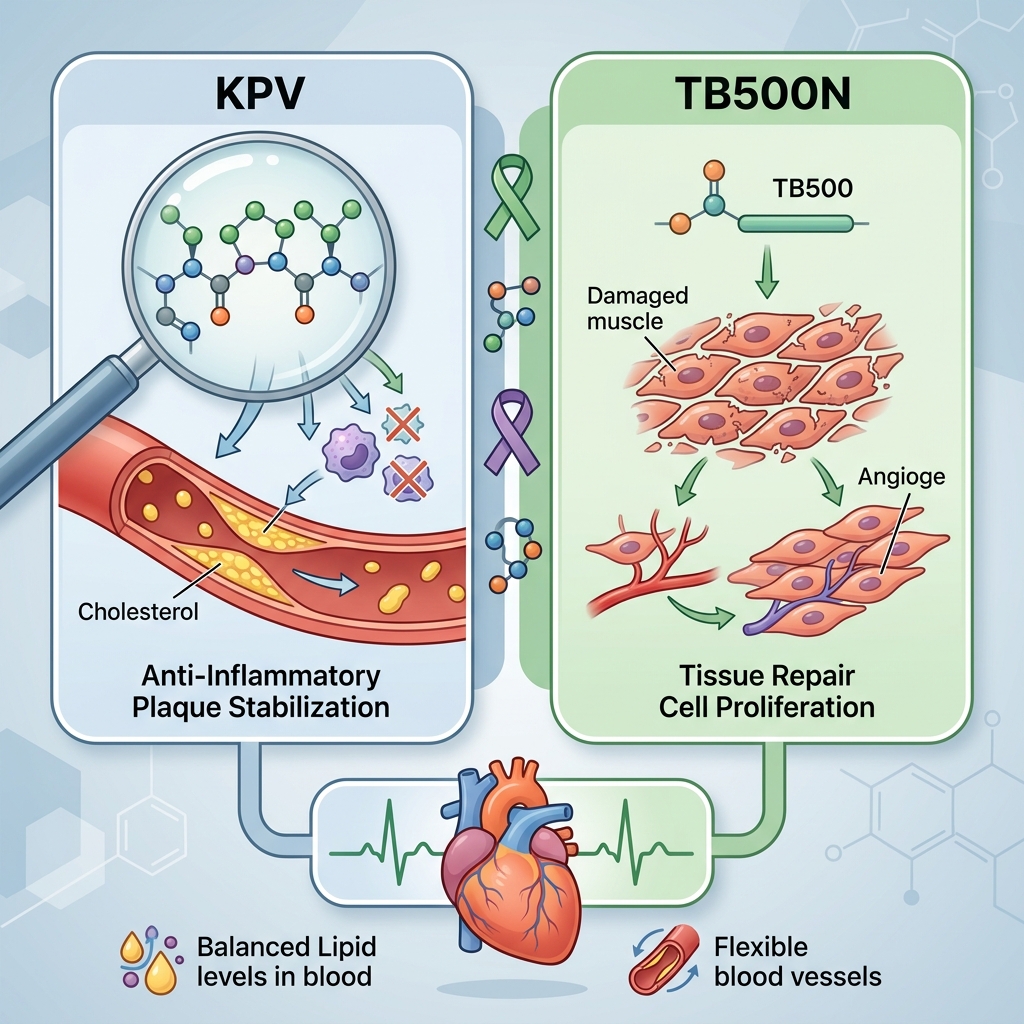
KPV is a tripeptide (Lysine-Proline-Valine) derived from the C-terminal sequence of alpha-MSH (alpha-melanocyte-stimulating hormone). It has demonstrated potent anti-inflammatory properties, particularly in suppressing NF-kB signaling — the very molecular pathway that TNF-alpha activates to dismantle endothelial tight junctions. By modulating this pathway, KPV research suggests a mechanism for preserving endothelial barrier integrity and reducing the foundational trigger of the atherosclerosis cascade.
TB-500 (Thymosin Beta-4 fragment) is a synthetic peptide known for its roles in tissue repair, cellular migration, and — critically — angiogenesis and endothelial regeneration. Research into TB-500 points to its potential to support the healing of damaged vascular tissue, reduce cardiac fibrosis, and improve functional recovery following ischemic events. Its anti-inflammatory profile complements KPV's NF-kB suppression, potentially creating a synergistic effect on vascular health at both the preventive and restorative levels.
Together, these peptides represent a research-driven approach that targets the actual mechanism of cardiovascular disease — systemic inflammation and endothelial dysfunction — rather than a downstream biomarker like LDL cholesterol.
Key Takeaways
- 60% of heart attack patients have normal cholesterol levels, according to data from the Framingham Heart Study
- Elevated CRP (C-reactive protein), a marker of systemic inflammation, is a stronger predictor of cardiovascular death than LDL cholesterol — by a factor of 2.3x
- Inflammation — driven by cytokines like TNF-alpha, IL-6, and IL-1 beta — breaks down the endothelial barrier, allowing LDL to enter arterial walls and initiate atherosclerosis
- Without chronic inflammation, LDL cannot infiltrate the arterial wall; atherosclerosis requires inflammation as its prerequisite
- Plaque rupture and heart attacks are caused by MMP-mediated fibrous cap thinning — a direct consequence of inflammatory activity within the plaque
- Symptoms like fatigue, ED, and brain fog may be early indicators of vascular inflammation and endothelial dysfunction
- KPV may help preserve endothelial integrity by suppressing NF-kB inflammatory signaling
- TB-500 may support vascular tissue repair, reduce cardiac fibrosis, and promote endothelial regeneration
- Targeting systemic inflammation — rather than cholesterol alone — represents a more mechanistically sound approach to cardiovascular health based on current research
This content is for educational purposes only and is not medical advice. The information presented here is intended to support independent research and should not be used as a substitute for professional medical evaluation, diagnosis, or treatment. Always consult a qualified healthcare provider before making any changes to your health regimen, medications, or supplement protocols. Peptides discussed in this article are research compounds and their use in humans may be subject to regulatory restrictions in your jurisdiction.
Shop Featured Peptides
Explore high-quality research peptides. Use our referral link to support independent research.